Biliary Atresia Associated with Polysplenia Syndrome,
Situs Inversus Abdominus, and Reverse Rotation of Intestine
Authors: Bilal Mirza,* Shahid Iqbal, Afzal Sheikh
APSP J Case Rep 2012;
3 (2): 14
Affiliation: Department of
Pediatric Surgery, The Children’s Hospital and the Institute of Child Health
Lahore, Pakistan.
Address
for Correspondence*: Dr. M. Bilal Mirza, 428 Nishter Block Iqbal Town Lahore,
Pakistan.
Email: blmirza@yahoo.com
Submitted
on: 12-01-2012
Accepted
on: 18-04-2012
Citation:
Mirza
B, Iqbal S, Sheikh A. Biliary atresia associated with polysplenia syndrome,
situs inversus abdominus, and reverse rotation of intestine. APSP
J Case Rep 2012; 3: 14.
Dear Sir
In 25% of cases of biliary atresia associated
malformations are present; polysplenia constitute 10-50% of these associated anomalies.
Biliary atresia found associated with polysplenia syndrome, heterotaxy, and
reverse rotation of intestine, in isolation or in various combinations; however
its association with polysplenia syndrome, situs inversus abdominus, and
reverse rotation of gut in the same patient is not reported in English language literature [1,2].
A 2-month-old female infant presented with jaundice, clay
colored stools, and abdominal distension since the first week of life. She was
a product of consanguineous marriage and born via normal vaginal delivery. General
physical examination revealed a vitally stable infant with obvious jaundice and
abdominal distension. Abdominal examination revealed hepatomegaly. Her
laboratory investigations showed conjugated hyperbilirubinemia (total bilirubin
14 mg/dl, and direct bilirubin 8 mg/dl). Gallbladder was not visualized on
ultrasound of the abdomen. On HIDA scan no excretion of the radiopharmaceutical
tracer was noted. At operation the gallbladder was found atretic (Fig. 1); per-operative
cholangiogram confirmed extrahepatic biliary atresia. The liver was enlarged
and central in position. Stomach and two big spleens (non-floating) were
present on the right side of the abdominal cavity (Fig. 1). The duodenum was
entirely intra-peritoneal and transverse colon was retroperitoneal in position (Fig.
2).

Figure 1: Showing atretic gallbladder (AG); stomach (St)
and two spleens (S) on right side; and intraperitoneal duodenum (D).
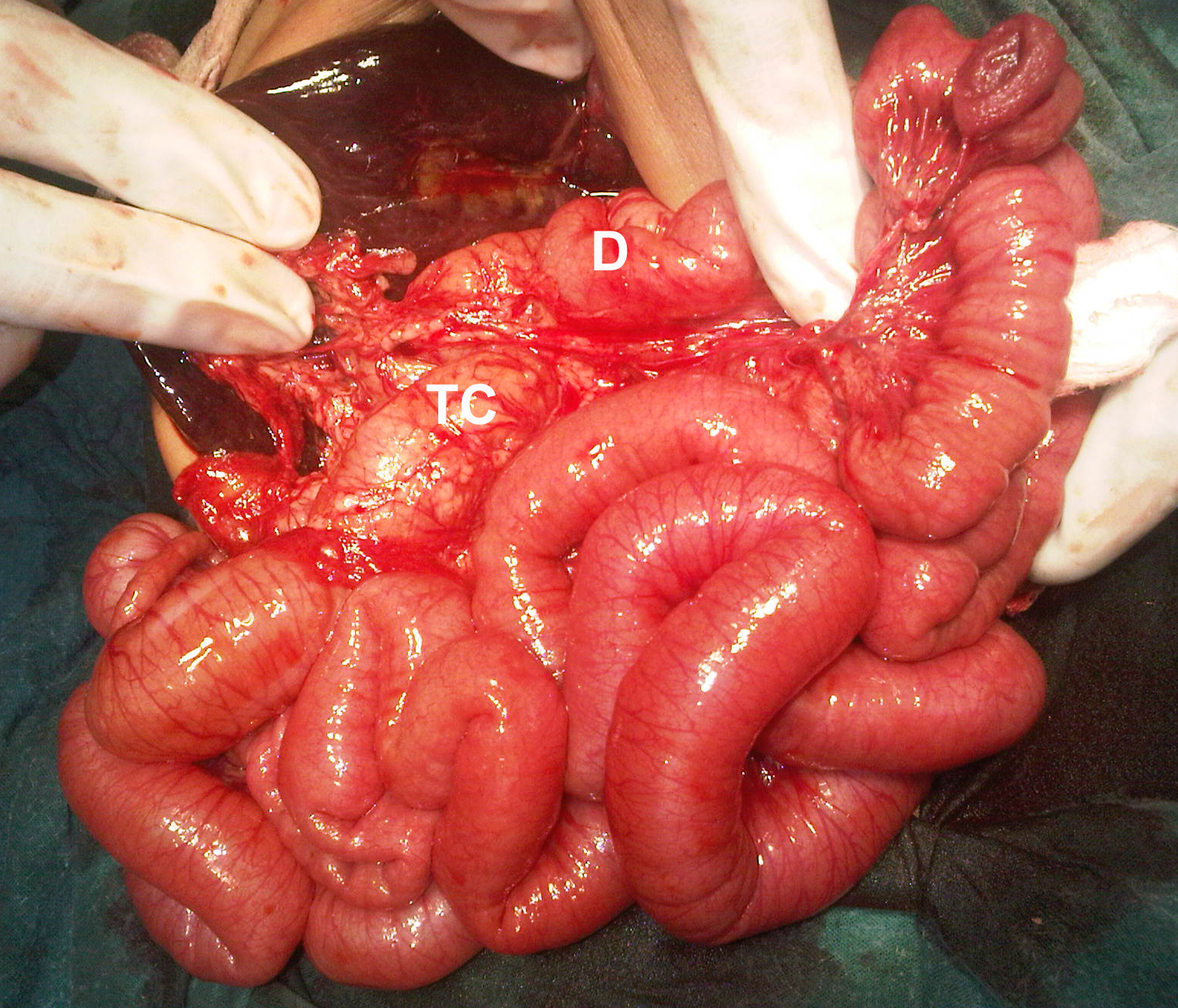
Figure 2: Showing intraperitoneal duodenum (D) and
retroperitoneal transverse colon (TC).
The atretic gallbladder and portal plate were dissected meticulously. Roux-en Y
hepatico-jejunostomy was performed without going through the transverse colon
window. Both the spleens were left as such. No effort was made to correct
reverse rotation. The postoperative recovery was uneventful. Patient was
allowed oral feeding on 5th
day of operation and discharged on 7th day. Liver biopsy showed
early cirrhotic changes. Postoperatively, echocardiography and chest x-ray did
not show intrathoracic heterotaxy. She was on follow up of gastroenterology
department for further management.
Polysplenia syndrome is associated with a number of
anomalies i.e. heterotaxy of abdominal or thoracic organs, malrotation of gut,
biliary atresia, reverse rotation of gut, intestinal atresia, retroperitoneal
teratoma, vena caval anomalies, cardiac, and lung anomalies. Few case reports
described the association of biliary atresia with polysplenia syndrome, situs
inversus, and immotile cilia syndrome. Polysplenia syndrome is more frequently
associated with vascular and cardio-pulmonary anomalies however the work of
Chandra proved that a subclass of patients of polysplenia syndrome had biliary
atresia that were associated with gastrointestinal and respiratory anomalies [1-3].
The abdominal heterotaxy in
a case of biliary atresia has few surgical implications. These problems are
related to the orientation of roux-en-y loop. In a usual case of biliary
atresia, the roux-en-y loop is passed through a rent made in the mesentery of
transverse colon, however in case of malrotation and reverse rotation of gut the
there could be difficulties in the orientation of the roux-en-y loop. This
difficulty is further incremented by mirrored anatomy of abdominal viscera. In
our case the stomach and spleens were lying on right side of the abdomen. The
duodenum was intraperitoneal and transverse colon retroperitoneal, therefore
mesentery of transverse colon was not available. Thus we have to take the
roux-en-y loop directly to the portal plate for hepatico-jejunostomy. To conclude,
biliary atresia polysplenia syndrome is a rare occurrence. The operating
surgeon must be aware of the surgical implications that may occur in case of
associated malrotation/reverse rotation, and mirrored alimentary tract anatomy.
References
1. Rasool F, Mirza B. Polysplenia syndrome associated with situs inversus
abdominus and type I jejunal atresia. APSP J Case Rep 2011;2:18.
2. Chandra RS. Biliary atresia and other structural
anomalies in the congenital polysplenia syndrome. J Pediatr
1974;85:649-55.
3. Emmanuel J, Danièle C, Nicole
R, Michelle H. CFC1 Gene Mutation and Biliary Atresia With
Polysplenia Syndrome. J Pediatr Gastroenterol
Nutrit 2002;34:326.