A Case of Fetus in Fetu
Authors: Ghulam Mustafa,* Bilal Mirza, Shahid Iqbal, Afzal Sheikh
APSP
J Case Rep 2012; 3(2): 9.
Affiliation: Department of
Paediatric Surgery, The Children's Hospital and the
Institute of Child Health Lahore, Pakistan.
Address for Correspondence*: Dr. Ghulam Mustafa, Department
of Paediatric Surgery, The Children's Hospital and the
Institute of Child Health Lahore, Pakistan.
E-mail: missyou009@yahoo.com
Submitted on: 14-03-2012
Accepted On: 12-04-2012
Citation: Mustafa G, Mirza B, Iqbal S, Sheikh A. A case of fetus in fetu. APSP J Case Rep 2012; 3: 9.
Abstract
Fetus
in fetu is a rare developmental aberration, characterized by encasement of partially
developed monozygotic, diamniotic, and monochorionic fetus into the normally
developing host. A 4-month-old boy presented with abdominal mass. Radiological
investigations gave the suspicion of fetus in fetu. At surgery a fetus enclosed
in an amnion like membrane at upper retroperitoneal location was found and
excised. The patient is doing well after the operation.
Keywords: Fetus in fetu, Teratoma, Abdominal mass.
Introduction
Fetus
in fetu (FIF) is an uncommon pathology that results due to abnormal embryogenesis in a diamniotic
monochorionic twin pregnancy with an incidence of 1 in 500000 births. The
commonly accepted theory states that unequal division of blastocoele results in
monozygotic, monochorionic, and diamniotic twins of unequal sizes following
which the smaller twin encases into the normally developing twin; the mechanism
of which is not known. This is followed by arrest of further growth of the
encased fetus due to improper blood supply or inherent defects of the encased
twin. Few authors consider FIF as an advanced form of teratoma [1-3]. We report
another case of fetus in fetu diagnosed preoperatively with the help of
radiological investigations.
Case report
A
4-month-old male baby presented to our hospital with the complaint of palpable
mass in the right hemi-abdomen noted by the parents one day back. The patient
was born at full term with uneventful birth history. The baby achieved milestones
normally. Abdominal examination revealed a non-tender mass with vague margins
in the right hemi-abdomen. Laboratory investigations including alpha-fetoprotein
were within normal limits. X-ray abdomen showed mass impression pushing the gut
shadows to one side. Bones and calcifications were also evident in the right
hemi-abdomen. Ultrasound of the abdomen revealed a heterogeneous mass with
calcifications suggestive of teratoma. Abdominal CT scan showed a 9.2cm × 10.0cm
heterogeneous mass containing fat, bones and soft tissues. The various bones
were vertebrae, long bones like femur, tibia and fibula, and bones of hand/feet
(Fig.1). Provisional diagnosis of FIF was made.

Figure 1: CT scan showing various kind
of bones in FIF.
At
operation, a mass covered in whitish-gray membrane, pushing the gut loops to
the opposite side in the upper retroperitoneum, was found (Fig.2). The membrane
was incised to find a fetiform mass floating in clear fluid having a few well
differentiated and other rudimentary organs. The fetiform mass was suspended in
the amnion like cavity with an umbilical cord like stalk (Fig.3). The mass with
sac was mobilized and excised completely.

Figure 2: Amnion like covering of FIF.
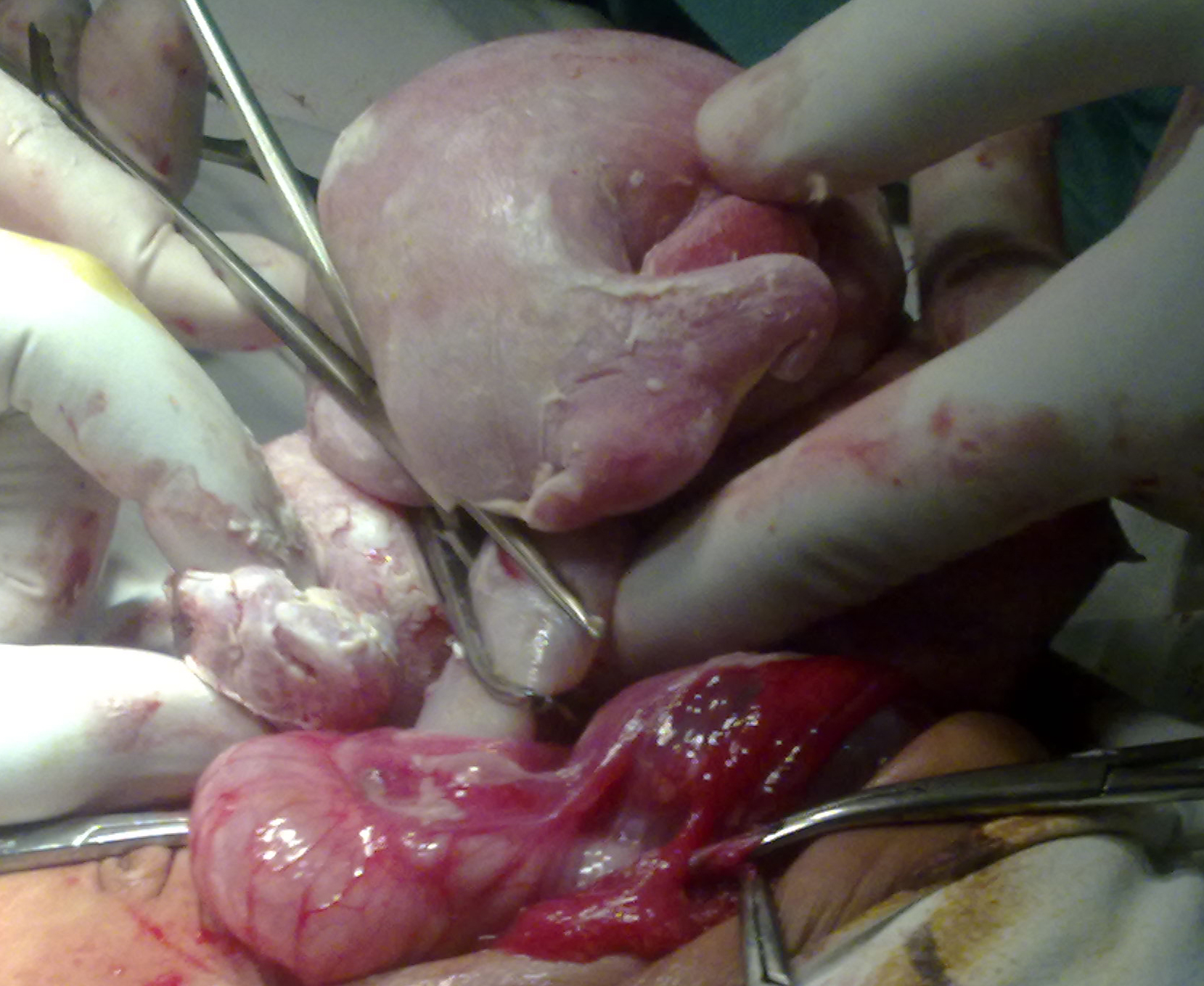
Figure 3: Umbilical cord like stalk- attachment of FIF.
Post
operative recovery was uneventful. Patient was allowed orally on 3rd and
discharged on 7th post operative day. The patient is currently being followed
with alpha-fetoprotein and ultrasound abdomen. At six months follow up patient is
doing well.
The
FIF was of 13.75cm×12.5cm×6.25cm size with a weight of 500 grams. It was
anencephalic having otic and nasal placodes and optic vesicles. The left upper
limb was meromelic; lower limbs were sirenomelic. The umbilical cord had two
vessels in it. The FIF had a scrotum like skin at the site of genitalia that
lacked gonad in it. The FIF also lacked anus and genitalia (Fig.4). Plain
radiography of the specimen revealed axial skeleton in the form of vertebrae,
along with ribs, long bones of upper and lower limbs, and facial bones (Fig.5).
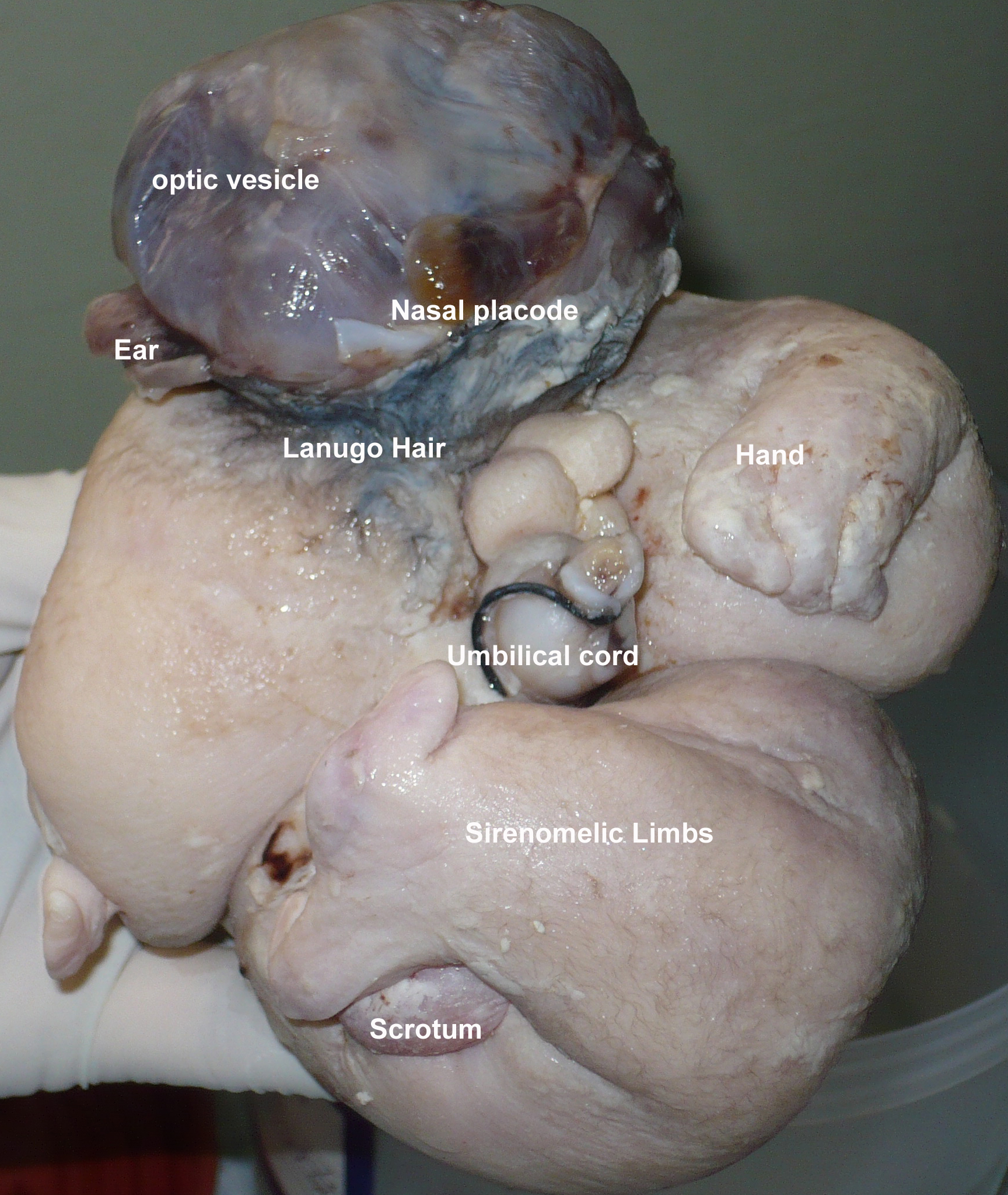
Figure 4: Various features of FIF.

Figure 5: Radiograph of FIF showing ribs, vertebrae, hip
bone, bones of face and limbs.
Discussion
The
term Fetus in fetu was coined by Meckel during the late 18th century following
which Willis described it as a rare condition where a malformed parasitic twin is
found encased in the host especially in the retroperitoneal space. The other
reported sites are abdomen, scrotum, cranium, kidneys, adrenals, mediastinum,
and lymph nodes etc. FIF usually occurs as a single lesion however multiple FIF
have also been reported, highest being 5. FIF is always a curiosity and to date
about 200 cases have been reported in literature [3-6].
Most
of the cases present during infancy, but late presentation has also been
reported with the oldest patient presenting at 47-year. Male preponderance is
noted in the reported cases. The major presenting complaint is a palpable
abdominal mass, predominantly in upper abdomen. The other symptoms are
secondary to the mass effect of the FIF such as, jaundice, hydronephrosis,
intestinal obstruction, meconium peritonitis, respiratory distress, and
vomiting [7-9].
Few
reports describe antenatal diagnosis of FIF. Preoperative diagnosis can be made
on plain radiographs and CT scan/MRI. The presence of vertebrae, long bones,
bones of hands and feet etc are the common radiological findings. Visualization
of a non-homogenous mass with bones especially vertebrae is considered
pathognomonic of FIF. Failure to visualize vertebrae however does not rule out
possibility of FIF. The other frequent differential is teratoma [1,5,10].
Most
of the reported cases describe FIF suspended with an umbilical cord like stalk
in an amnion like membrane containing fluid- equivalent to amniotic cavity. In
few cases, the exact blood supply could be identified; in most of cases the
blood supply was thought to come from the abdominal wall where amnion like membrane
was in close approximation to it. Similarly, in our case the FIF was suspended
in the fluid filled cavity with an umbilical cord like structure having two
vessels in it. The FIF are usually
anencephalic, with the vertebrae and limb-buds (long bones and bones of
hands/feet can also present), and acardiac (rarely heart was found). In few
cases vertebral column was not found however presence of mature enteric nervous
plexi and melanocytes in the skin depicted the fetus
would have passed the primitive streak stage of notochord development [1-5]. In
our case the FIF was anencephalic, having primitive structures of nose, eyes
and ears. One hand was well developed. The lower limbs were fused as in
sirenomelia- long bones were palpable in the lower limbs.
Careful
dissection of FIF should be done to avoid injury to the surrounding structures.
A case of bile duct injury has been reported in literature. Complete excision
of FIF along with covering membrane is necessary, as a case of malignant
transformation of left over membrane is reported in literature. These cases are
monitored with alpha-fetoprotein or beta-HCG, along with ultrasound and other
radiological investigations [11,12]. We are following
our patient on similar lines.
References
1. Eng
HL, Chuang JH, Lee TY, Chen WJ. Fetus in fetu: a case report and review of the
literature. J Pediatr Surg 1989;24:296-9.
2. Bader
I, Akhter N, Sajjad M, Khalid
A, Khan N, Anwar ul Haq. Twin
fetus in fetu - a very rare entity: A case report with review of literature.
Pak J Med Sci. 2003;19:306-9.
3. Gangopadhyay AN,
Srivastava A, Srivastava P,
Gupta DK, Sharma SP, Kumar V. Twin fetus in fetu in a child: a case
report and review of the literature. J Med Case Reports. 2010;4: 96.
4. Luzzatto C, Talenti E, Tregnaghi A, Fabris S, Scapinello A, Guglielmi M. Double fetus in fetus: Diagnostic imaging. Pediatr Radiol 1994;24:602-3.
5. Federici S, Ceccarelli PL, Ferrari M, Galli
G, Zanetti G, Domini R. Fetus in fetu. Report of
three cases and review of the literature. Pediatr
Surg Int 1991;6:60-5.
6. Gunaydin M, Celik FC, Tander B, Bozkurter AT, Sullu Y, Baris S, et al. Two cases of fetus in fetu. J Pediatr Surg 2011; 46: e9-e12.
7. Kim
YJ, Sohn SH, Lee JY, Sohn
JA, Lee EH, Kim EK, et al. Misdiagnosis of fetus-in-fetu as meconium peritonitis.
Korean J Pediatr 2011;54:133-6.
8. Singh
S, Rattan K, Navtej, Gil M, Mathur
SK, Sen R. Fetus-in-fetu presenting as
acute intestinal obstruction. Indian J Pathol Microbiol 2010;53:128-9.
9. Singh
SN, Partap A, Sinha AK, Kumar A, Lakshmi
R, Shakya UC. Giant retroperitoneal fetus in fetu: An
unusual case of respiratory distress. J Indian Assoc Pediatr
Surg 2007;12:158-60.
10. Kurdi AM,
Al-Sasi OM, Asiri SM, Al-Hudhaif JM. Fetus-in-fetu. Imaging and
pathology. Saudi Med J 2012;33:444-8.
11. Joshi
M, Parelkar S, Shah H, Agrawal A, Mishra
P. Foetus in fetu with common
bile duct injury: a case report and review of literature. ANZ
J Surg. 2009;79:651-2.
12. Hopkins
KL, Dickson PK, Ball TI, Ricketts RR, O'Shea PA, Abramowsky
CR. Fetus-in-fetu with malignant recurrence. J Pediatr
Surg 1997;32:1476-9.