Duodenal Duplication Cyst having Ectopic Gastric and Pancreatic Tissues
Authors: Binod Kumar Rai,* Samina Zaman1, Bilal Mirza, Ghazala Hanif1,
Afzal Sheikh
APSP J Case Rep 2012; 3(2): 15.
Affiliation: Departments of Pediatric Surgery and Histopathology1,
The Children’s Hospital & the Institute of Child Health Lahore, Pakistan.
Address for Correspondence*: Dr. Binod K Rai, Department of Pediatric
Surgery, The Children’s Hospital and the Institute of Child Health Lahore,
Pakistan.
Email: binod_50@hotmail.com
Submitted on: 25-02-2012
Accepted on: 20-03-2012
Citation: Rai BK, Zaman S, Mirza B, Hanif G, Sheikh A.
Duodenal duplication cyst having ectopic gastric and pancreatic tissues. APSP J
Case Rep 2012: 3: 15.
A 1-year-old female child
presented with distention of abdomen, accompanied with occasional episodes of vomiting
and abdominal pain for the past eight months with no history of constipation or
fever. The child was vitally stable. On inspection upper abdomen was found distended
and mild tenderness in epigastrium on deep palpation. Laboratory investigations
were within normal limits. The plain radiograph of abdomen was unremarkable.
Ultrasound scan showed a 6.9 cm x 7.5 cm sized cystic area with internal debris
at porta hepatis, compressing the liver. CT scan showed a 5 cm x 7 cm sized
cyst extending from porta hepatis to the duodenum (Fig. 1). The preoperative
differentials were duodenal duplication and choledochal cyst.
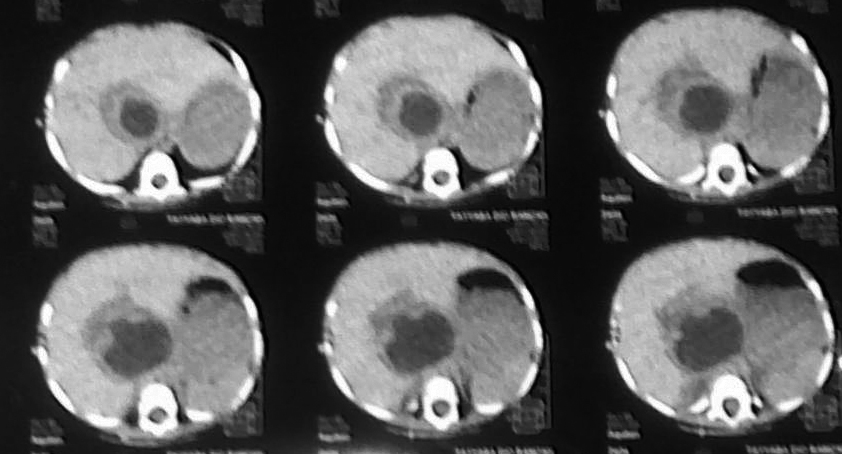
Figure 1: CT scan showing a hypo-dense
area at porta hepatis.
At operation, a cyst medial
to the gall bladder, pushing the stomach and the pancreas anteriorly and
intimately related to the second part of the duodenum was found (Fig. 2).The
content of the cyst was clear mucous on aspiration. Intra-operative cystogram
was performed that ruled out its communication with biliary and alimentary
tracts (Fig. 3). The wall of the cyst was opened and stripping of mucosal
lining performed after excising resectable portion of the cyst. The cyst was
sharing common wall with duodenum and was non - communicating. The child made
an uneventful recovery and was discharged on the fifth postoperative day.
Histopathology of the specimen showed gastric mucosal lined tissue having
smooth muscles in the wall along with ectopic pancreatic tissue (Fig. 4,5).
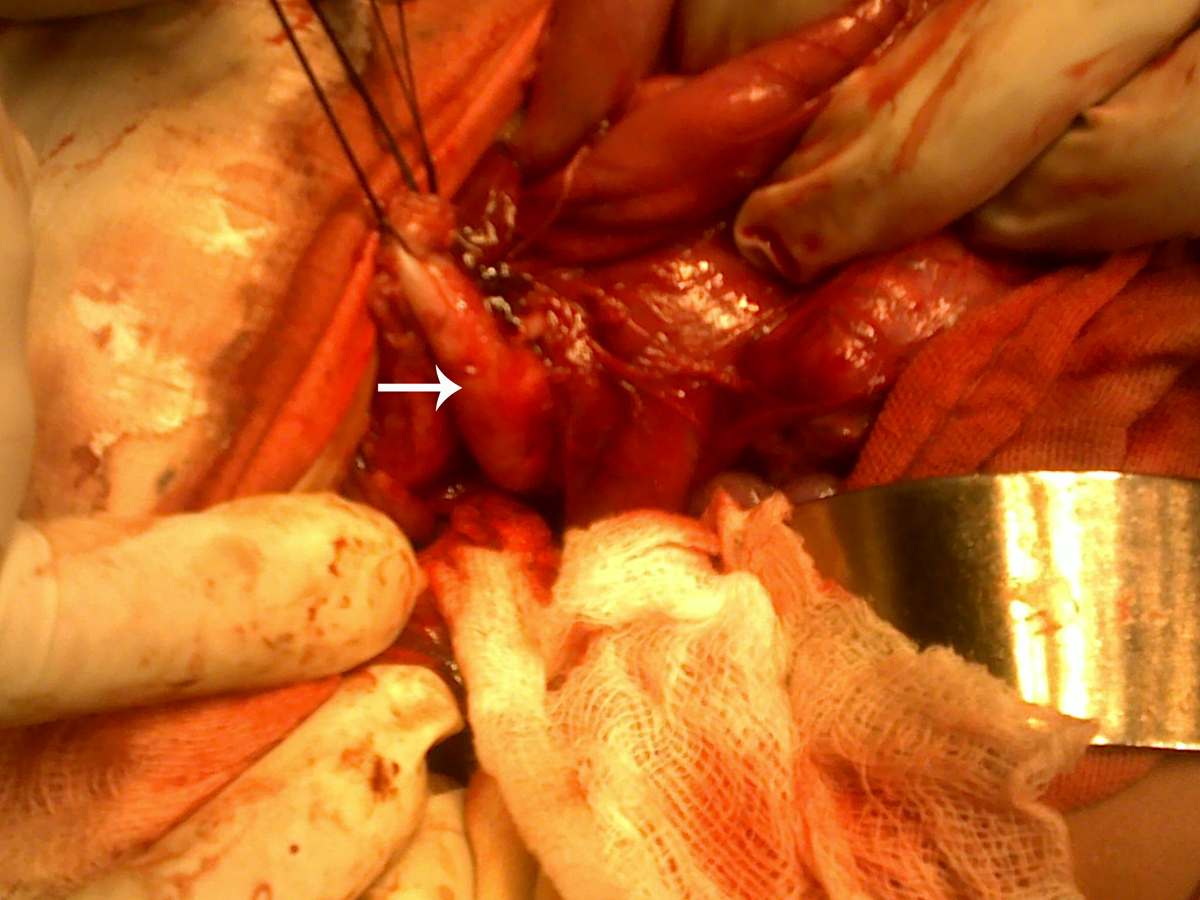
Figure 2: Dissection of the duodenal duplication cyst (Arrow).
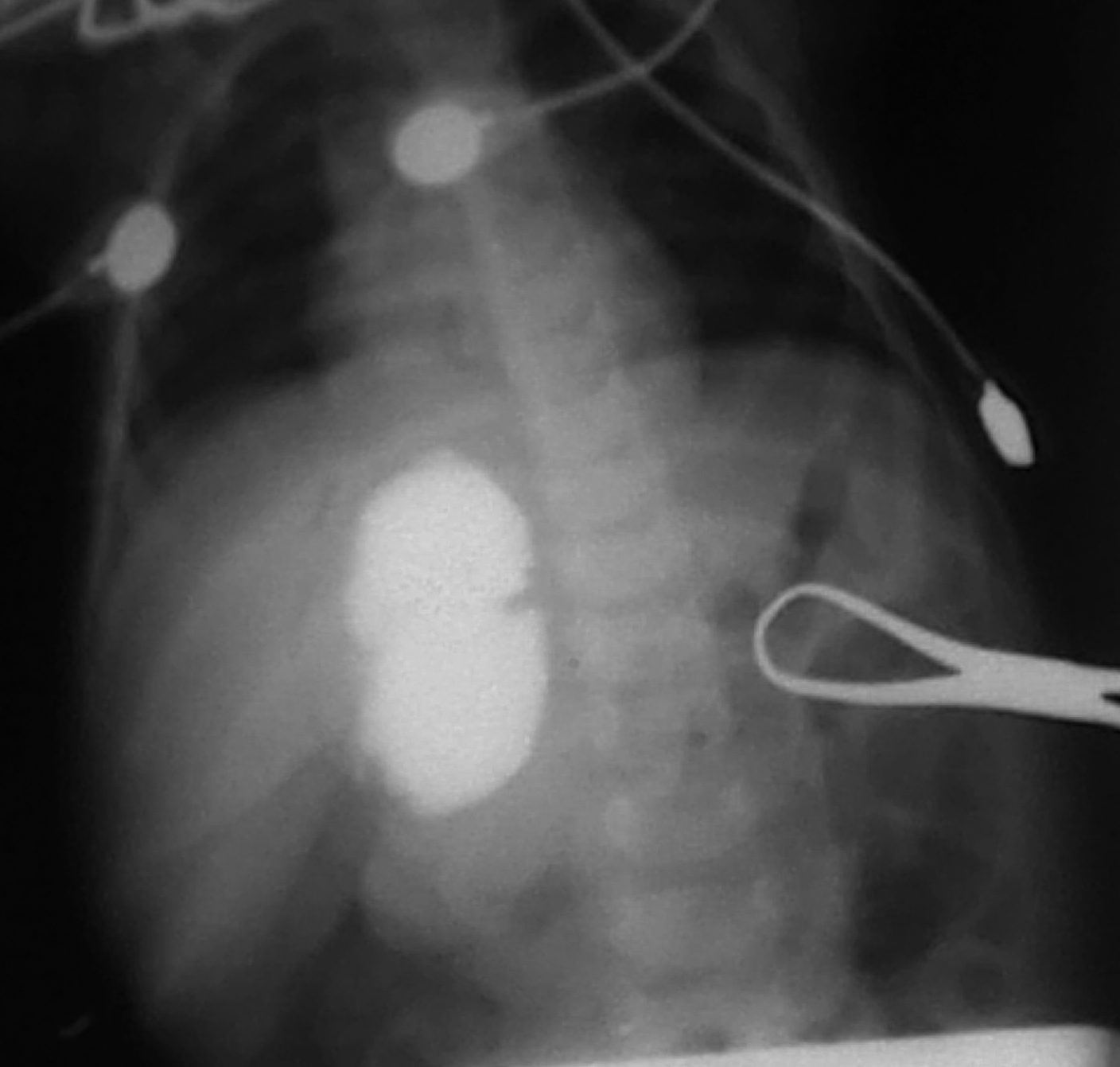
Figure 3: Intra-operative
cystogram showing no communication with pancreatico-biliary ducts and duodenum.
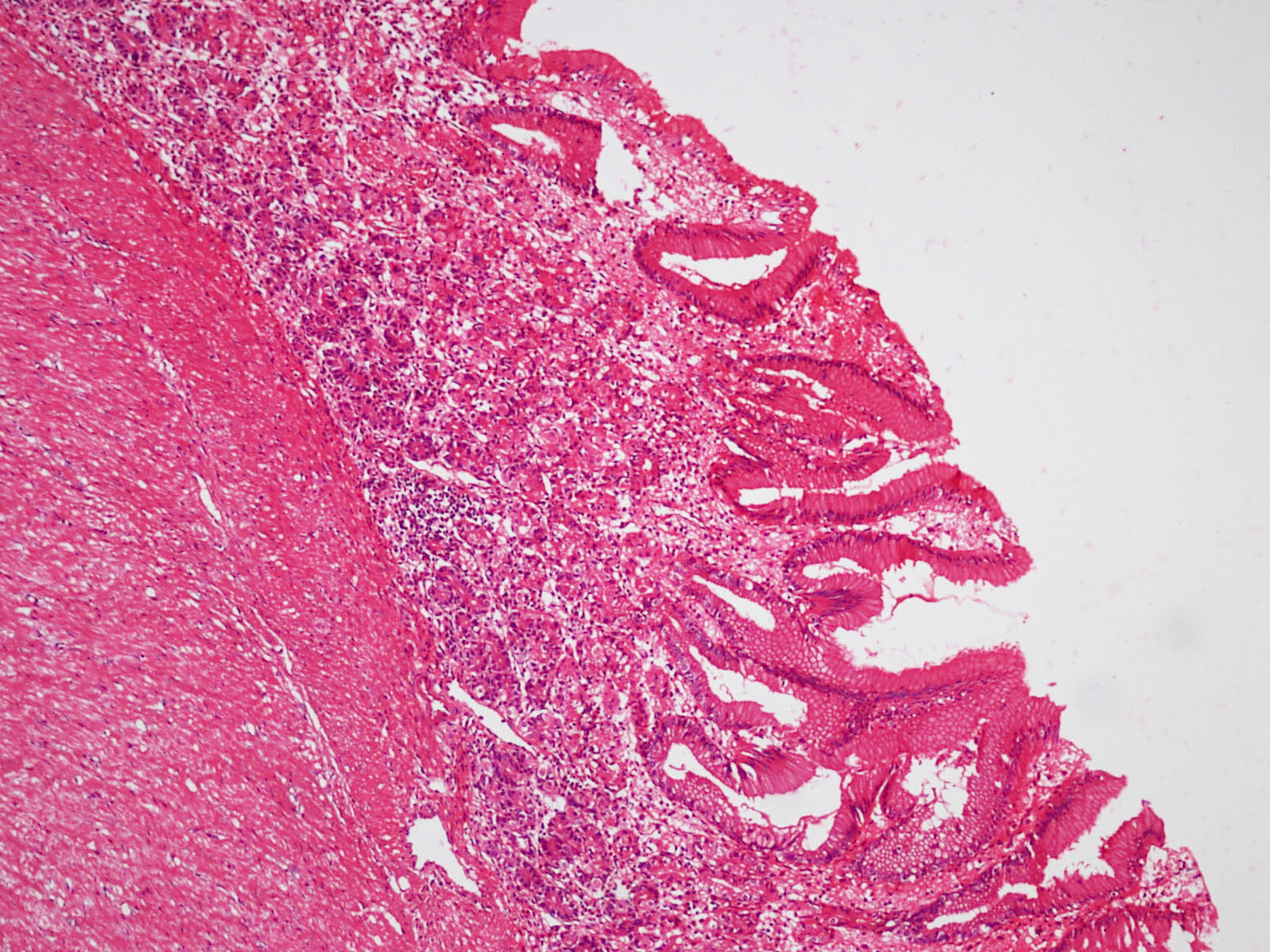
Figure 4: Microphotograph showing
gastric mucosa with underlying muscle layer (x200).
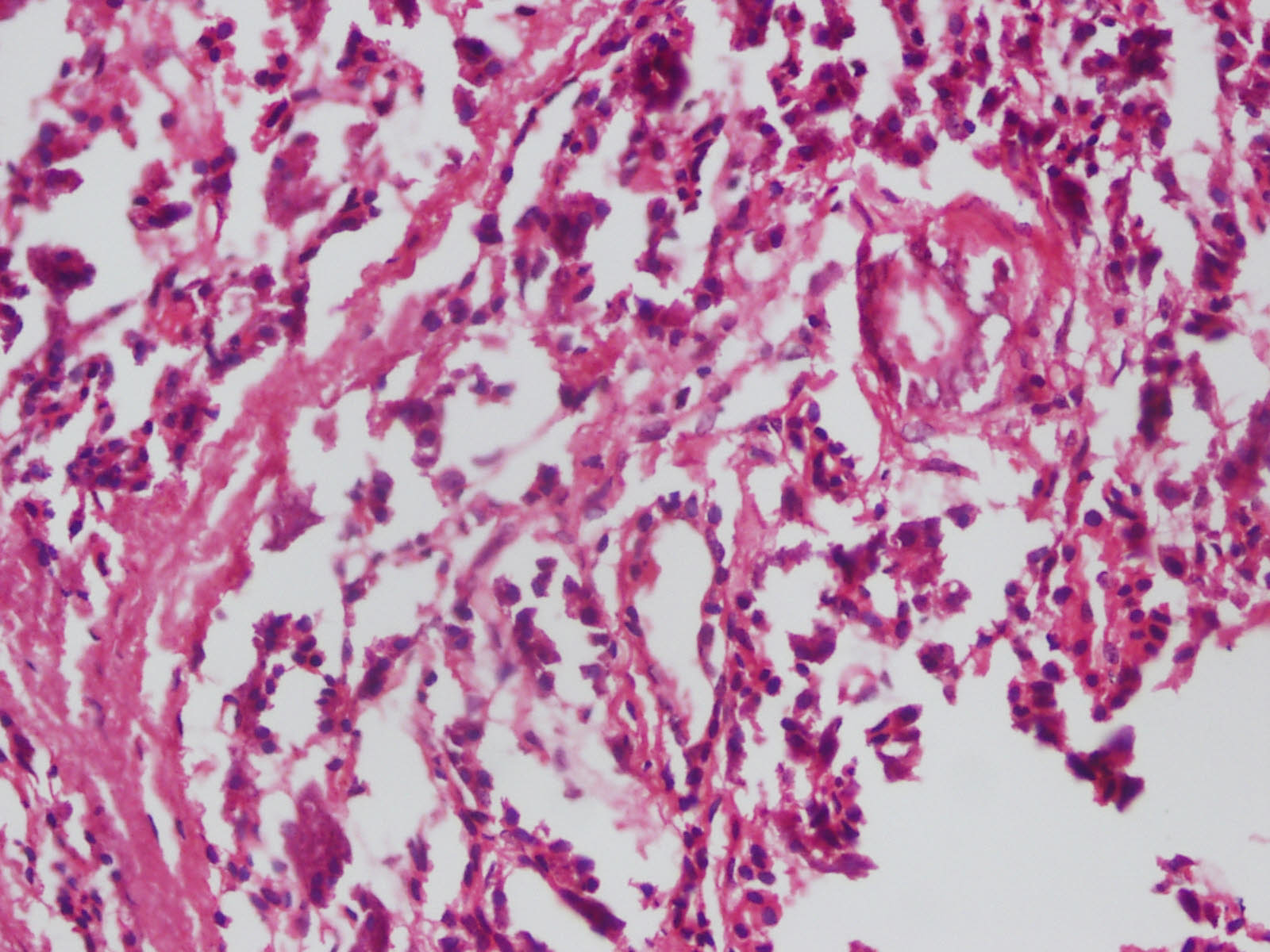
Figure 5: Microphotograph
showing pancreatic tissue (x400).
Discussion
Gastrointestinal
duplications may be cystic or tubular in shape with an intimate contact with
the adjacent gut, smooth muscles in their wall, and mucosa resembling that of
gastrointestinal tract. Duplications can present along any part of
gastrointestinal tract, commonly along the ileum; duodenal duplications account
for 5% of all gastrointestinal duplications. In 15-25% of cases ectopic gastric
mucosa may be found. Few cases of duodenal duplications containing ectopic
pancreatic tissue have been reported in literature. Concurrence of ectopic gastric
and pancreatic tissues in a duodenal duplication cyst, as found in the index
case, is however extremely rare [1-3].
Duodenal duplications may
occur along the first and second parts of duodenum and are cystic with no
communication with the intestinal lumen in most of the cases. Rarely, they can
arise from pancreatico-biliary ducts. These cysts may be confused with
choledochal cysts on account of their location between porta hepatis and
duodenum. The presentation could be with abdominal pain, palpable epigastric
mass, relapsing pancreatitis, and vomiting. In case of ectopic gastric mucosa,
there could be intra-cystic hemorrhage or perforation of the cyst with
peritonitis [2,3].
Ultrasound scan, upper
gastrointestinal contrast study, CT scan, magnetic resonance cholangio pancreatography
(MRCP), and endoscopy are important tools for preoperative diagnosis. Surgical
resection is the treatment of choice for alimentary tract duplications. However,
in case of duodenal duplications, excision of as much as part of duplication
and mucosal stripping of the rest is preferred on account of its close
proximity with pancreatico-biliary ductal systems. We proceeded on the same
lines in our patient. Intra-operatic cystogram is mandatory to rule out its
communication with pancreatico-biliary tree. Similarly, we have ruled out the
communication of the cyst with pancreatico-biliary system and gut lumen by
performing intra-operative cystogram. Drainage of the duplication cysts into
the duodenum or into a Roux limb of jejunum is also an acceptable alternative
[1-4].
References
1.
Lund DP. Alimentary tract duplications. In: O’Neill JA, Rowe MI, Grosfeld
JL, Fonkalsrud WE,
Coran AG. Editors. Pediatric
Surgery, 6th ed,
Philadelphia: Mosby, 2006:1389-99.
2.
Narlawar RS,
Rao JR, Karmarkar SJ, Gupta
A, Hira P. Sonographic findings in a duodenal
duplication cyst. J Clin Ultrasound 2002; 30:566-8.
3.
Lavine JE,
Harrison M, Heyman MB. Gastrointestinal duplications
causing relapsing pancreatitis in children. Gastroenterol
1989; 97:1556-8.
4.
Irani S, Kozarek R, Mason V. Duodenal Duplication Cysts: A rare, but
treatable cause of relapsing pancreatitis. Am J Gastroenterol
2009;104:S60-1.