Reconstructive Surgery in a Patient with
Persistent Cloaca
Authors: Altaf Begum, Afzal Sheikh*, Bilal Mirza
APSP
Journal of Case Reports 2011; volume 2 (3): 23
Address:
Department of Pediatric Surgery, The Children’s Hospital and the Institute of Child
health Lahore, Pakistan
Email:*
profafzalsheikh@yahoo.com
Date of Submission:
12-07-11
Date of Acceptance:
24-08-11
Citation: Begum A,
Sheikh A, Mirza B. Reconstructive surgery in a patient with persistent cloaca.
APSP J Case Rep 2011;2:23
Abstract
Cloacal malformations
are challenging as to the surgical correction. A case of cloacal
malformation who underwent reconstructive
surgery is being reported. The patient had colostomy in the neonatal period and
reconstruction was performed at the age of 6 year. The
surgical management included abdomino-perineal anorecto-urethro-colo-vaginoplasty.
The
patient is fully continent of urine and achieved fair continence of feces
at 9 months of follow up.
Key words:
Persistent cloaca, Urogenital sinus, Anorectal
malformation, Fecal continence.
Introduction
Persistent cloaca is an uncommon malformation
with a wide spectrum of urogenital and hind gut anomalies. It is
placed under the heading of complex/rare malformations in the Krickenbeck’s
classification of anorectal malformations [1]. The clinical presentation is of
imperforate anus with a single perineal opening through which urine and
meconium are passed. Unlike other anorectal malformations, surgical treatment
is demanding as urinary and fecal incontinence are
frequently reported following operation. The ultimate goal of treatment
includes achieving satisfactory bowel and urinary control as well as normal
sexual functions at maturity [1-3]. In this manuscript the management of the
index anomaly is reported who achieved normal urinary and fair fecal
continence.
Case Report
A six-year-old female presented for
definitive procedure of persistent cloaca (Fig. 1). She had colostomy on 5th
day of life. Ultrasound of abdomen was
reported as normal. Distal colostogram showed high
recto-cloacal fistula (Fig. 2).
Endoscopic evaluation revealed an opening at bladder neck. At operation anal sphincter was identified by
nerve stimulation and dissection started by making anterior sagittal
incision. The sites for the future vagina and ano-rectum were made. Abdomen was
then opened by mobilizing the stoma. Urinary bladder was opened and ureteric
catheterization done to avoid their damage during surgery. The anomaly was
identified as high confluence of rectum and vagina opening into the cloaca at
the level of bladder neck (Fig. 3). The opening of vagina was very minute that
could not be identified on endoscopy as well as at operation. Distal loop of
the colon was mobilized and detached from common cloaca. It was tailored
distally, to be used as vaginal substitute and pulled down at the perineum,
while its proximal end anastomosed with lower end of the vagina that was about
1/3rd in length. Similarly proximal loop of colon mobilized to bring
it down as ano-rectum, through the already identified site for anus. Feminizing
clitoroplasty was added. The common channel was left as urethra. Finally
perineal body was constructed (Fig. 4). Patient had uneventful recovery.

Figure 1: Preoperative
figure showing single perineal opening.
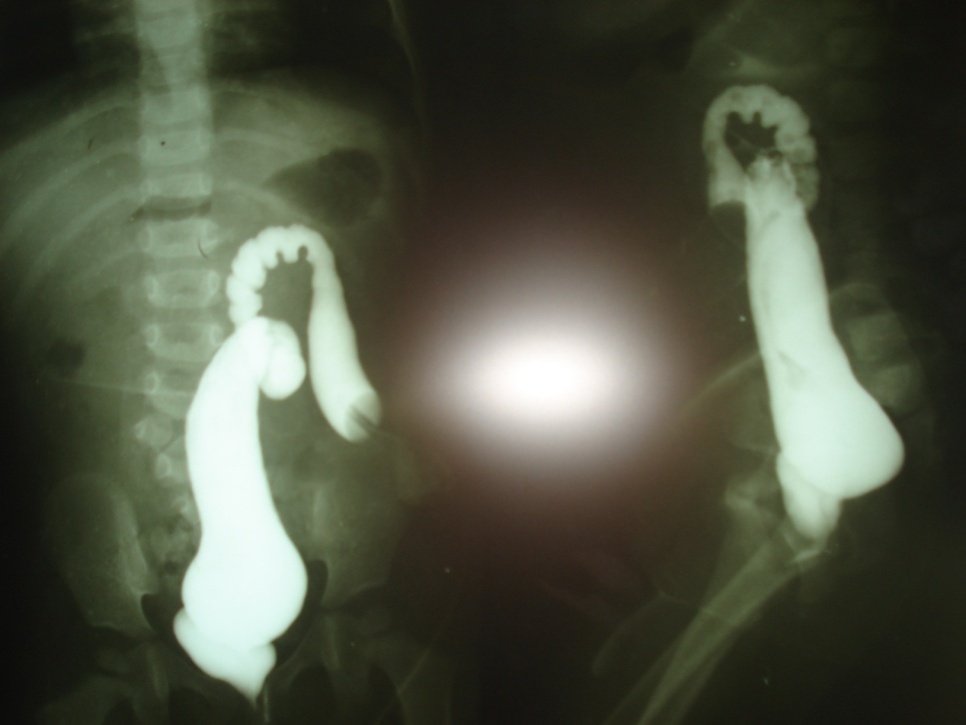
Figure 2: Distal loopogram showing high insertion of rectum
into common channel.

Figure 3: Illustration of
the cloacal malformation

Figure 4 3:
Postoperative showing anorecto-colovagino-urethroplasty.
Examination done after 02 weeks of surgery
showed healed patent vaginal and anal passages. On 10th week post
operative visit, the mother was satisfied the urinary continence.
She observed occasional soiling (Kelly’s continence score 3). She was on follow
up and on vaginal dilatation program.
Discussion
Common cloaca or persistent cloaca is rare
congenital malformation characterized by confluence of rectum, vagina and the distal
urinary tract into a single common channel. Cloacal anomalies
occur in 1:250,000 live births [1]. Management of
these defects is a challenge to pediatric surgeons. The
definitive treatment in most centers is a single stage reconstruction
though some surgeons opt for repairing the anorectal
anomaly initially and leave urogenital sinus repair for later date. The
surgical management is planned after carefully identifying the anatomy
specially measuring length of common channel, level of insertions of urinary
channel, vagina and rectum, and associated urogenital anomalies.
The patients with cloacal malformations are
categorized in two groups depending upon the length of the common channel. Those having common channel shorter than 3cm (more than 60% of
entire group) can be repaired by posterior sagittal approach. The second
group has a length of the common channel more than 3cm where the total
urogenital mobilization from perineum will not be enough to repair
the malformation, so the common channel is left intact to be used as urethra,
and colovaginoplasty along with anorectoplasty is performed as done in our case
[3-5].
Fecal and urinary incontinence is a major
problem in high variety anorectal malformations. Their intensity is even higher
in cases of persistent cloaca. Almost 60% patients have incontinence of variable
degrees. The incidence is usually higher in cases of higher confluence where an
abdomino-perineal approach is used [1,5]. In our case
despite extensive pelvic and perineal dissection the patient achieved fair
bowel and normal urinary control. This may be
attributed to the well developed perineal muscles and sparing
of the urethral sphincter along
with good surgical repair.
Acknowledgements: We are thankful to
Miss Fatima Ijaz (PhD Organic Chemistry) for making the illustration of the
cloacal malformation in our case.
References
1.
Buhilla P, Torres PC, Bruned BJ, Emparan G, DeSalazar C, Castro
LC. Total mobilization of the urogenital sinus in the treatment of cloaca. An Esp Pediatr 2001;55: 573-5.
2.
Kay
R, Tank ES. Principles of management of persistent cloaca in the female
newborn. J Urol 1977;117:102-4.
3.
Masuko T, Higashimoto Y, Iwai J.
Single-stage operation without temporary colostomy for persistent cloaca with
short common channel. Pediatr Surg
Int 2005;21:922-4.
4.
Malik
A, Iqbal Z, Hameed S, Khalid C, Iftikhar A, Hussain M.
Persistent cloaca with complete duplex ectopic ureters:
A rare presentation. J Med Rehabilit 2007;1:7-9.
- Levitt MA, Pena A. Pitfalls in the
management of newborn cloacas. Pediatr
Surg Int 2005;21:264-9.